MRI Explained for Prostate Cancer Part1
Excerpts from my Diary
Reaction from a Nurse.
The question by the nurse surprised me in a big way. The question was, What are you taking for medication without a prescription from the doctor? I was thinking what kind a question is that, my answer was Ivermectin, clear and with no hesitation. Later I realized why she was asking me that question in the first place. She noticed that my PSA number was going down from 9.3 to 5.53, that is a 40.5% reduction of the cancer. With that kind of reduction, I had to take something against the cancer. On my documentation from the hospital, I took no medication at all. So I had to take something without a prescription from my doctor. Than she asked me if it was OK to write it into my records that I was taking Ivermectin. That was OK with me at that time.
Norby
Excerpts from my Diary
Now the doctors reaction.
Later the doctor came into the room, we made small talk, after that I told him that I took Ivermectin. His reaction was interesting. First of all he did not know that the latest PSA number came down from 9.3 to 5.53. I felt like he was indifferent to the result, meaning he did not praise the result nor did he condemn it. I do not believe him, that he did not know the PSA number, because he looked at the same documents on the computer like the nurse did, so he also saw the PSA number came down. I also gave him a copy of my writings, so he gets a better understanding of my thinking why I do not want the operation or the radiation as my first option of action.
Norby
Results of my MRI explained.
Exam Description:
MRI Prostate with and without IV Contrast
1. MRI with and without IV Contrast
Excerpt:
Over the past few years, multiparametric MRI (mpMRI) of the prostate has emerged as the most successful radiologic imaging study for detecting prostate cancer. The PI-RADS system and the MRI pathway have paved the way for a widespread usage of this imaging test in daily clinical practice [1]. Prostate MRI is on the verge of opening up further indications towards screening, which is quite remarkable. As a result, the number of prostate MR scans has increased sharply and this trend will continue in the next years. This puts pressure on the justification to perform the most invasive and “controversial” part of MRI of the prostate, the dynamic contrast-medium-enhanced sequence.
2. Gadolinium-based contrast agents (GBCAs)
Excerpt:
Gadolinium contrast agents- challenges and opportunities of a multidisciplinary approach: Literature review.
Contrast agents is used in magnetic resonance imaging (MRI) to improve the visibility of the details of the organ structures. Gadolinium-based contrast agent (GBCA) has been used since 1988 in MRI for diagnostic and follow-up of patients, the gadolinium good properties make it an effective choice for enhance the signal in MRI by increase its intensity and shortening the relaxation time of the proton.
Clinical history:
Biopsy-proven prostate cancer, Gleason score 3+4=7, on active surveillance.
Most resent PSA: 5.86 ng/mL on 02/16/2026.
If available, previous MRI information is compared with the current MRI to see the current changes. In my case we have the Gleason score and the latest PSA number.
Technique:
Multisequence multiplanar MR imaging of the prostate gland was performed on a 3 Tesla magnet. Precontrast 3-plane high-resolution T2-weighted images, axial T1-weighted images, and axial diffusion weighted images with ADC maps of the prostate were obtained. Axial T1, T2, and fat-suppressed T2-weighted images of the whole pelvis were obtained. Dynamic post contrast imaging of the prostrate gland was performed following administration of 12ml Dotarem intravenously. Post processing and gland segmentation was performed on a DynaCAD workstation.
1. Multisequence multiplanar MR imaging
Excerpt:
Multiparametric-magnetic resonance imaging (mp-MRI) has shown promising results in diagnosis, localization, risk stratification and staging of clinically significant prostate cancer. It has also opened up opportunities for focal treatment of prostate cancer. Combinations of T2-weighted imaging, diffusion imaging, perfusion (dynamic contrast-enhanced imaging) and spectroscopic imaging have been used in mp-MRI assessment of prostate cancer, but T2 morphologic assessment and functional assessment by diffusion imaging remains the mainstay for prostate cancer diagnosis on mp-MRI. Because assessment on mp-MRI can be subjective, use of the newly developed standardized reporting Prostate Imaging and Reporting Archiving Data System scoring system and education of specialist radiologists are essential for accurate interpretation.
2. Precontrast 3-plane high-resolution T2-weighted images
Excerpt:
Physics
A T2WI relies upon the transverse relaxation (also known as “spin-spin” relaxation) of the net magnetization vector (NMV). T2-weighting tends to require long TE and TR times.
One way to think about T2 relaxation is as follows:
after an RF excitation pulse, there is relaxation of the spins from the transverse plane toward the main longitudinal magnetic vector (B0) – this is T1-weighting
at the same time, spins are decaying from their aligned precession in the transverse plane – differences in this decay are captured on T2-weighting
3. Axial T1-weighted images,
Excerpt:
Unlike imaging using radiation, in which the contrast depends on the different attenuation of the structures being imaged, the contrast in MR images depends on the magnetic properties and number of hydrogen nuclei in the area being imaged. Different contrasts in the area being imaged can be selected for by running different sequences with different weightings. The main three sequences are:
- T1-weighted (maximum T1 contrast shown)
- T2-weighted (maximum T2 contrast shown)
- Proton density (PD) weighting (density of hydrogen protons shown)
4. Axial diffusion weighted images
Excerpt:
Abstract
For assessing a cancer treatment, and for detecting and characterizing cancer, Diffusion-weighted imaging (DWI) is commonly used. The key in DWI’s use extracranially has been due to the emergence of of high-gradient amplitude and multichannel coils, parallelimaging, and echo-planar imaging.
5. ADC maps of the prostate were obtained
Excerpt:
Synopsis
A method for simultaneous T1, T2 and Apparent Diffusion Coefficient (ADC) mapping, STimulated-Echo based Mapping (STEM), has been proposed to achieve rapid and co-registered multi-slice T1, T2 and ADC maps within a moderate scan time. In this study, the STEM method is optimized for prostate imaging and evaluated in 16 patients with suspected prostate cancer (PCa) or benign prostatic hyperplasia (BPH). T1, T2 and ADC maps were successfully estimated and compared among BPH, PCa and healthy prostate tissues.
6. Axial T1, T2, and fat-suppressed T2-weighted images of the whole pelvis were obtained
Excerpt:
MRI interpretation
T1 v T2 images
Key points
- On T1 images FAT is white
- On T2 images both FAT and WATER are white
It’s all about FAT and WATER
The two basic types of MRI images are T1-weighted and T2-weighted images, often referred to as T1 and T2 images.
The timing of radiofrequency pulse sequences used to make T1 images results in images which highlight fat tissue within the body.
The timing of radiofrequency pulse sequences used to make T2 images results in images which highlight fat AND water within the body.
So, this makes things easy to remember.
T1 images – 1 tissue type is bright – FAT
T2 images – 2 tissue types are bright – FAT and WATER
7. Dynamic post contrast imaging
Excerpt:
Dynamic Contrast-Enhanced MRI (DCE-MRI) is a powerful imaging sequence that adds a functional dimension to prostate cancer diagnosis. While T2-weighted imaging provides detailed anatomical views and Diffusion-Weighted Imaging (DWI) reveals cellular density, DCE-MRI visualizes tumor vascularity and tissue perfusion. By tracking how a contrast agent moves through the prostate, this technique helps radiologists characterize
8. 12ml Dotarem intravenously
Excerpt:
Structured Product Label
The following Structured Product Label (SPL) was submitted to the FDA by Guerbet Llc for the product Dotarem (NDC 67684-3001). This document serves as the official prescribing information, containing essential scientific data and clinical materials required for healthcare providers and patients.
This specific version of the label includes detailed information regarding warning: nephrogenic systemic fibrosis (nsf), 1 indications and usage, 2 dosage and administration, 2.1 dosing guidelines, 2.2 drug handling, 3 dosage forms and strengths, 4 contraindications, 5.1 nephrogenic systemic fibrosis, and other regulatory disclosures. Use the navigation below to review specific sections of the FDA submission.
9. Post processing and gland segmentation
Excerpt:
The impact of pre- and post-image processing techniques on deep learning frameworks: A comprehensive review for digital pathology image analysis
Findings:
Prostate:
Measurement: 5.2×3.7×4.8cm. Estimated volume: 47.4 cc, previously 37.2 cc. PSA density 0.12 ng/ml/cc, previously Prostatic density: 0.24 ng/mL2.
Quality: Motion degrades image quality and limits evaluation.
Postbiopsy hemorrhage: None.
Peripheral zone: Multifocal linear and wedge-shaped T2 attenuation of the peripheral zone likely related to scarring and/or sequela of prostatitis.
Transition zone: Multiple heterogeneous nodules consistent with prostatic hyperplasia.
1. Estimated volume: 47.4 cc, previously 37.2 cc
Excerpt:
What is a Normal Prostate Volume?
In healthy adult males, the normal prostate gland measurement is approximately:
Width: 1.6 inches (4 cm)
Height: 1.2 inches (3 cm)
Depth (thickness): 1 inch (2.5 cm)
This results in a prostate that weighs about 0.7 to 1 ounce or 20 to 30 grams. The total prostate volume is 20 to 30 cubic centimeters (cc). For comparison, that’s about the size of a walnut.
Its size allows the prostate to carry out its primary function, which is to produce seminal fluid that nourishes sperm and supports ejaculation.
2. What can be done to reduce volume?
I am looking for an answer. A 27% increase in volume is not good. the question is: What can be done to reduce the size and or to slow down the growth naturally?
I am still looking for results.
Norby
3. PSA density change from 0.24 to 0.12 ng/ml/cc
Excerpt:
Understanding PSA Density and Prostate Cancer
What is PSA Density?
Prostate-specific antigen (PSA) density is calculated by dividing the PSA level by the prostate volume. This metric helps assess the risk of prostate cancer more accurately than PSA levels alone. A higher PSA density indicates a greater likelihood of prostate cancer, while a lower density suggests a lower risk.
Impact of Lower PSA Density
Prognosis: Men with lower PSA density generally have better survival rates. This is because lower density often correlates with less aggressive forms of prostate cancer.
Treatment Decisions: Patients with lower PSA density may require less aggressive treatment options. This can include active surveillance rather than immediate intervention.
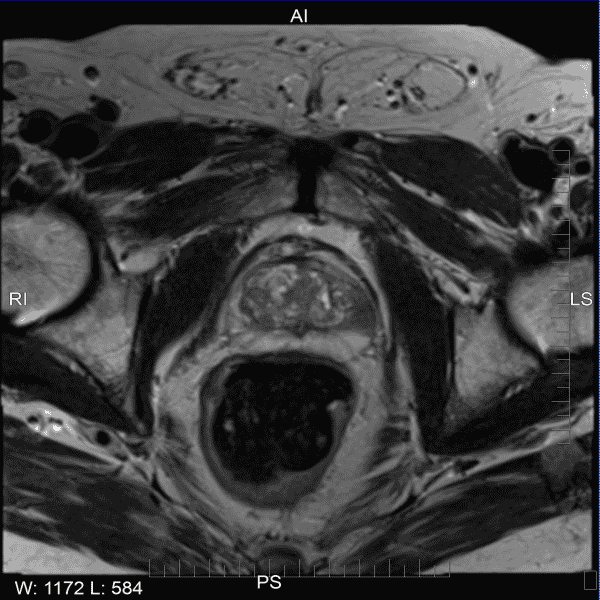
MRI Evaluations
Focal Lesions:
Lesions #1:
Locations: Left, anterior peripheral zone midgland to base.
Size: 10 mm (series 4 image 17), previously 5 mm.
T2: Score 4. Heterogeneous moderate hypointensity.
DWI/ADC: Score 3. Moderately hyperintense on DWI and markedly hypointense on ADC.
Mean ADC value -0.655 x 10-3 mm2/s.
DCE: Positive.
Extraprostatic extension: Equivocal. Board capsular contact is present.
PI-RADS score: 4. PIRADS 4 High (clinically significant cancer is likely to be present).
Neurovascular bundle: Unremarkable
Seminal vesicles: Unremarkable.
Urinary bladder: Urinary bladder wall thickening, likely sequela of chronic outlet obstruction.
Rectum/Colon: There is colonic diverticulosis and increased stool in the colon.
Lymph nodes: No pathologically enlarged lymph nodes.
Bones: No aggressive osseous lesions.
Other: No significant pelvic free fluid. Small fat-containing left inguinal hernia.